Table of Contents
- What Are Brucella Antibodies?
- Why Brucella Antibodies Are Medically Important
- How the Brucella Antibody Test Is Performed
- The 5 Key Types of Brucella Antibody Tests Explained
- How to Read Your Brucella Antibody Test Results
- Who Must Get Tested for Brucella Antibodies?
- Treatment Decisions Based on Brucella Antibody Findings
- Frequently Asked Questions
- Trusted External Resources
Introduction
Brucella antibodies are the essential biological markers that healthcare professionals rely on to diagnose brucellosis, one of the most prevalent and dangerously underdiagnosed zoonotic infections in the world today.
When the body is exposed to Brucella bacteria through contaminated food, infected animals, or occupational hazards, the immune system mounts a defence by generating specific Brucella antibodies in the bloodstream. Detecting and measuring these antibodies is not simply a laboratory formality, it is often the only way to confirm a diagnosis that symptoms alone cannot provide.
Brucellosis earns the nickname ‘disease of a thousand faces’ because its symptoms, undulant fever, drenching night sweats, fatigue, and joint pain, overlap with dozens of other conditions. Without a Brucella antibody test, patients frequently go misdiagnosed for months.
What Are Brucella Antibodies?
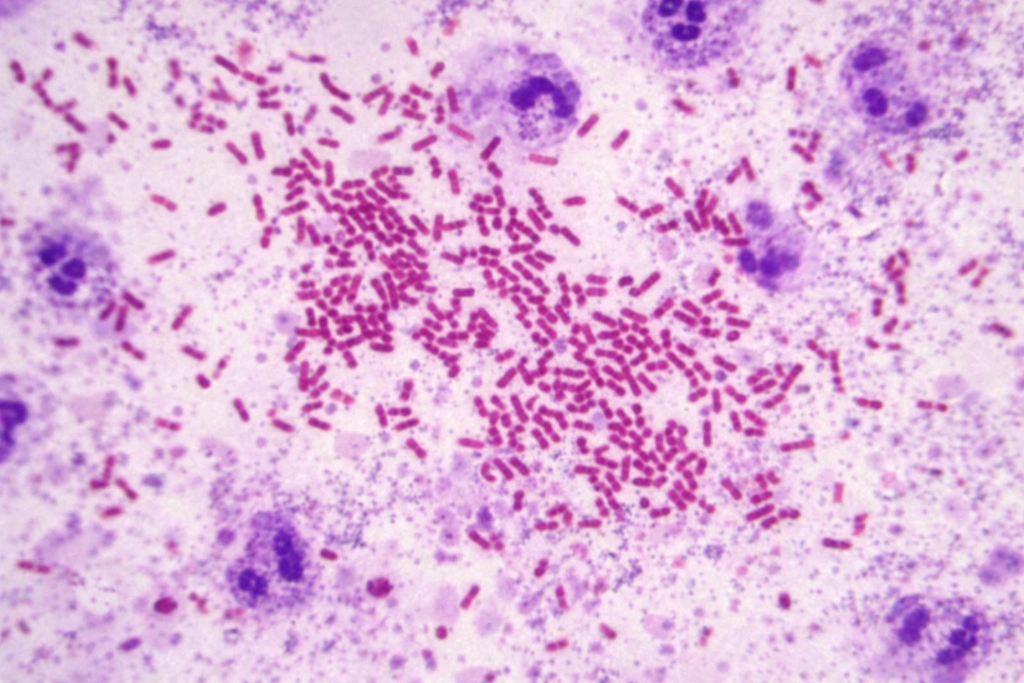
Brucella antibodies are immunoglobulin proteins produced by B-lymphocytes — white blood cells responsible for humoral immunity — in direct response to antigens found on the surface of Brucella bacteria. These antibodies are highly specific: they are manufactured to recognise and bind to Brucella surface lipopolysaccharide (LPS) and other outer membrane proteins.
There are two primary classes of Brucella antibodies that diagnostic laboratories measure:
- IgM brucella antibodies:The first responders. IgM antibodies appear within the first one to two weeks of infection, signaling an acute, early-stage exposure to Brucella. Their presence strongly suggests recent or ongoing active infection.
- IgG Brucella antibodies: The long-term markers. IgG antibodies develop several weeks after infection and can persist in the bloodstream for one to two years, even after successful antibiotic treatments. Elevated IgG levels indicate chronic infection, relapse, or a recently treated case requires monitoring.
- IgA Brucella antibodies detectable through ELISA in some patients are particularly relevant in cases of localized brucellosis affecting the gastrointestinal tract or reproductive organs.
The relative levels and combination of these three brucella antibody classes allow clinicians to construct a timeline of infection, determining whether the disease is in its acute, chronic, or resolution phase.
Why Brucella Antibodies Are Medically Important ?
Brucella bacteria are classified by the WHO as potential bioterrorism agents (Category B) due to their high infectivity through aerosol transmission, their ability to survive outside a host, and the severity of untreated disease. In endemic regions across the Middle East, Mediterranean, Central Asia, and Latin America, brucella antibody testing remains the primary population-level tool for detecting active cases.
From a clinical standpoint, the importance of brucella antibody testing cannot be overstated for several reasons:
- Blood cultures — the definitive confirmation method — require up to six weeks to yield results and demand biosafety level 3 laboratory conditions. Brucella antibody tests deliver results in hours to days in any equipped laboratory.
- Untreated brucellosis progresses to serious complications, including sacroiliitis, spondylitis (spinal infection), endocarditis, neurobrucellosis, and orchitis. Early detection through brucella antibody testing directly prevents these outcomes.
- In pregnant women, a positive brucella antibody result triggers immediate intervention — because brucellosis during pregnancy carries a significant risk of spontaneous abortion, intrauterine foetal death, and neonatal transmission.
Monitoring brucella antibody titres over time allows physicians to assess whether antibiotic treatment is working and whether a relapse is occurring — making the test valuable not only for diagnosis but for ongoing disease management.
How the Brucella Antibody Test Is Performed ?
The brucella antibody test is a straightforward blood-based investigation requiring no special preparation. Here is exactly what to expect:
- No fasting is required before a Brucella antibody test, though your doctor may combine it with other fasting blood tests in the same draw.
- A phlebotomist draws a venous blood sample — typically 5 to 10 ml — from a vein in your forearm. The procedure takes under two minutes.
- The blood is centrifuged to separate the serum, which contains the Brucella antibodies, from the cellular components.
- The serum is then tested using one or more of the methods described in the next section.
- Results are typically available within 24 to 72 hours for standard agglutination tests, and within 24 hours for rapid tests such as the Rose Bengal Plate Test.
A critical concept in Brucella antibody testing is the antibody titre — the highest dilution of serum that still produces a measurable reaction. Expressed as a ratio (e.g., 1:80, 1:160, 1:320), the titre reflects the concentration of Brucella antibodies in the blood. Higher titres generally indicate a more robust immune response and, in the appropriate clinical setting, more active disease.
The 5 Key Types of Brucella Antibody Tests Explained
A. Rose Bengal Plate Test (RBPT) Rapid Screening
The RBPT is the most widely used first-line rapid screening tool for Brucella antibodies globally. A drop of rose Bengal-stained Brucella abortus antigen is mixed with patient serum on a white card. Visible agglutination (clumping) within four minutes indicates the presence of Brucella antibodies and is recorded as a positive screen. The RBPT is highly sensitive but has lower specificity, meaning false positives can occur. Any positive result must be confirmed by a quantitative test.
B. Standard Agglutination Test (SAT) the Quantitative Gold Standard
The SAT — also known as the Wright agglutination test — is the classical quantitative method for measuring Brucella antibody titres. Serial dilutions of patient serum are mixed with a standardised Brucella antigen suspension. The titre is the highest dilution at which visible agglutination still occurs. A titre of 1:160 or above is internationally recognised as diagnostically significant in a symptomatic patient. The SAT measures both IgM and IgG Brucella antibodies together.
C. 2-Mercaptoethanol (2-ME) Test Differentiating IgM from IgG
The 2-ME test is performed in conjunction with the SAT to distinguish between IgM and IgG Brucella antibodies. The chemical 2-mercaptoethanol selectively destroys IgM antibodies by breaking their disulfide bonds. If the SAT titre drops significantly after 2-ME treatment, the brucella antibodies present were predominantly IgM — consistent with acute infection. If the titre remains elevated after treatment, IgG brucella antibodies are the main component, indicating chronic or relapsing disease.
D. Enzyme-Linked Immunosorbent Assay (ELISA) Maximum Sensitivity
ELISA is the most sensitive and specific modern method for detecting and quantifying Brucella antibodies. Unlike agglutination-based tests, ELISA can individually measure IgM, IgG, and IgA brucella antibody classes in the same serum sample. This makes ELISA indispensable for diagnosing chronic brucellosis, where IgM may have declined, for monitoring treatment response through serial IgG measurements, and for detecting relapses where IgG levels rise again after initial decline. ELISA has become the preferred method in reference laboratories worldwide.
E. Coombs Anti-Human Globulin Test — Catching Hidden Brucella Antibodies
In a proportion of chronic brucellosis patients, brucella antibodies are present in a non-agglutinating form called blocking or incomplete antibodies, that the standard SAT cannot detect. This creates a dangerous false-negative result. The Coombs test adds anti-human globulin serum to the reaction mixture, which bridges these non-agglutinating Brucella antibodies and triggers visible agglutination. The Coombs test is essential when clinical suspicion remains high despite a negative or low SAT result.
How to Read Your Brucella Antibody Test Results
Interpreting Brucella antibody test results requires combining laboratory values with the patient’s clinical history, symptom duration, occupation, and risk factors. The table below summarizes the key interpretive framework:
Test | Result / Titre | Antibody Class | Meaning |
RBPT | Negative | — | No detectable brucella antibodies |
SAT | ≥ 1:160 | IgM + IgG | Active / recent brucellosis likely |
2-ME | Positive after 2-ME | IgG | Chronic or relapsing infection |
ELISA | High IgM | IgM | Acute / early stage |
ELISA | High IgG | IgG | Chronic / treated, monitor closely |
Coombs | Positive | Non-agglutinating IgG | Hidden antibodies — do not miss |
Important — Negative Does Not Always Mean Clear: If symptoms began fewer than seven days ago, the immune system may not yet have produced detectable levels of Brucella antibodies. A negative result in this window should always be repeated after two to three weeks if clinical suspicion remains. Similarly, very high antibody concentrations can occasionally produce a false-negative SAT through the ‘prozone effect’ the Coombs test resolves this.
Important : Positive Does Not Always Mean Active: Brucella antibodies, particularly IgG, can persist in the blood for 12 to 24 months after successful antibiotic treatment. A positive result in a previously treated patient does not automatically indicate active disease, rising titres on serial testing, combined with returning symptoms, are far more significant than a single positive value.
Who Must Get Tested for Brucella Antibodies ?
Testing for Brucella antibodies is clinically indicated across several well-defined risk groups. Early identification through targeted testing prevents disease progression and protects public health:
- Farmers, shepherds, cattle herders, and anyone with regular direct contact with livestock particularly goats, sheep, cattle, pigs, and camels in endemic regions.
- Veterinarians, veterinary nurses, and animal laboratory workers who handle animal tissue, blood, or abortion material from potentially infected animals.
- Slaughterhouse and meat-processing workers exposed to animal carcasses or offal on a daily basis.
- Consumers who have recently ingested unpasteurised milk, raw dairy products (including fresh goat or sheep cheese), or undercooked meat from endemic regions.
- Traveler’s returning from high-risk countries particularly in the Middle East, Mediterranean basin, Central Asia, sub-Saharan Africa, or Latin America presenting with fever of unknown origin.
- Any patient with unexplained fever lasting more than one week, especially when accompanied by night sweats, arthralgia, myalgia, hepatosplenomegaly, or lumbar pain.
- Pregnant women with any of the above risk factors brucella antibody testing is urgent in this population, given the severe obstetric consequences of untreated infection.
- Healthcare workers and laboratory personnel in brucellosis-endemic settings, or those who have experienced accidental exposure to Brucella specimens.
Treatment Decisions Based on Brucella Antibody Findings
A confirmed positive brucella antibody result interpreted alongside compatible clinical features initiates a structured treatment protocol. Brucellosis requires combination antibiotic therapy; monotherapy is associated with unacceptably high relapse rates of up to 40 percent.
First-Line Combination Regimens
- Doxycycline 100 mg twice daily for 6 weeks + Rifampicin 600–900 mg once daily for 6 weeks the standard WHO-recommended oral regimen for uncomplicated brucellosis.
- Doxycycline 100 mg twice daily for 6 weeks + Streptomycin 1 g intramuscularly once daily for 2–3 weeks, preferred for severe disease and associated with lower relapse rates than the doxycycline,rifampicin combination.
Trimethoprim-sulfamethoxazole (TMP-SMX) combined with rifampicin is the recommended regimen for children under 8 years of age, for whom doxycycline is contraindicated.
Special Populations
- Pregnant women: TMP-SMX combined with rifampicin throughout pregnancy, avoiding aminoglycosides in the first trimester and doxycycline throughout. Obstetric monitoring is essential.
- Neurobrucellosis: Extended treatment of 3 to 6 months using doxycycline, rifampicin, and a third agent (ceftriaxone or TMP-SMX) due to the difficulty of achieving bactericidal drug levels in the central nervous system.
- Brucella endocarditis: The most severe complication, often requiring surgical valve replacement in addition to prolonged antibiotic therapy for 3 to 6 months.
Monitoring Through Brucella Antibody Titres
- After initiating treatment, Brucella antibody titres are measured at 3-month intervals. A falling IgG titre alongside clinical improvement is reassuring. A plateau or rising titre, combined with returning symptoms, signals treatment failure or relapse and requires urgent reassessment. Relapse occurs in 5 to 15 percent of patients and is not caused by antibiotic resistance but by inadequate treatment duration or intracellular bacterial persistence.
Conclusion
Brucella antibodies are far more than a laboratory value on a report — they are the immune system’s precise, measurable record of its encounter with one of medicine’s most elusive bacterial pathogens.
Understanding which class of Brucella antibodies is elevated, by how much, and in what clinical context transforms a blood test result into an actionable diagnosis. Whether you are a patient experiencing unexplained fever, a clinician managing a complex zoonosis, or a public health professional monitoring endemic disease, the ability to correctly interpret brucella antibodies data is an indispensable clinical skill.
Early and accurate diagnosis through brucella antibody testing means earlier treatment, fewer complications, lower relapse rates, and better patient outcomes. If you have any risk factors for brucellosis, consult your doctor about Brucella antibody testing today. It could make all the difference.
Frequently Asked Questions
How long do Brucella antibodies remain detectable after treatment?
IgM brucella antibodies typically become undetectable within 3 to 6 months of successful treatment. IgG Brucella antibodies may persist for 12 to 24 months after cure. The continued presence of IgG alone, without clinical symptoms or a rising titre, does not necessarily indicate active disease — serial testing and clinical assessment together guide this interpretation.
What is the prozone effect in brucella antibody testing?
The prozone effect occurs when very high concentrations of brucella antibodies paradoxically block agglutination, producing a false-negative SAT result. It is more common in chronic, heavily infected patients. Laboratories overcome this by testing serum at higher dilutions or by using the Coombs test, which detects non-agglutinating Brucella antibodies and eliminates the prozone problem.
Can brucella antibodies disappear completely?
IgM disappears early, but IgG may persist for years.
Trusted External Resources on Brucella Antibodies
The following authoritative sources provide additional, peer-reviewed information on brucella antibodies and brucellosis:
World Health Organization — Brucellosis Fact Sheet (WHO.int)
Centers for Disease Control and Prevention — Brucellosis Overview (CDC.gov)
MedlinePlus — Brucella Antibody Test (medlineplus.gov)
PubMed — Brucella Antibody Diagnostic Research (pubmed.ncbi.nlm.nih.gov)
Medical Disclaimer:
This article is intended for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional with any questions regarding a medical condition.