Table of Contents
- What Is Thrombocytopenia in Pregnancy?
- How Common Is It?
- Causes of Thrombocytopenia in Pregnancy
- Signs and Symptoms to Watch For
- Risks for Mother and Baby
- Diagnosis
- Treatment Options
- Delivery Planning
- Frequently Asked Questions
1. What Is Thrombocytopenia in Pregnancy?
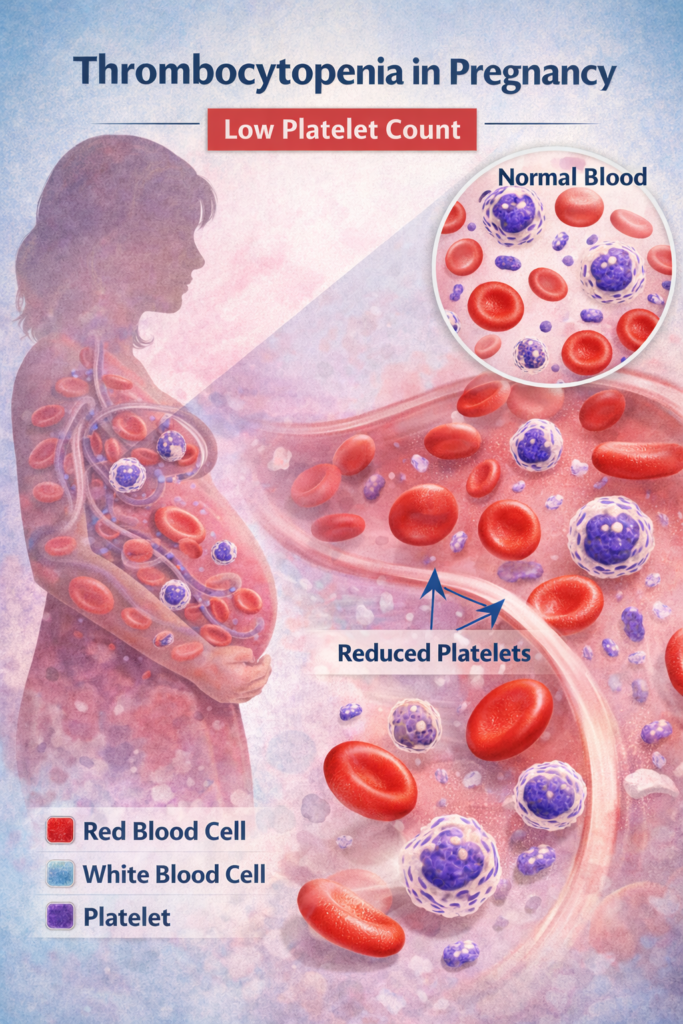
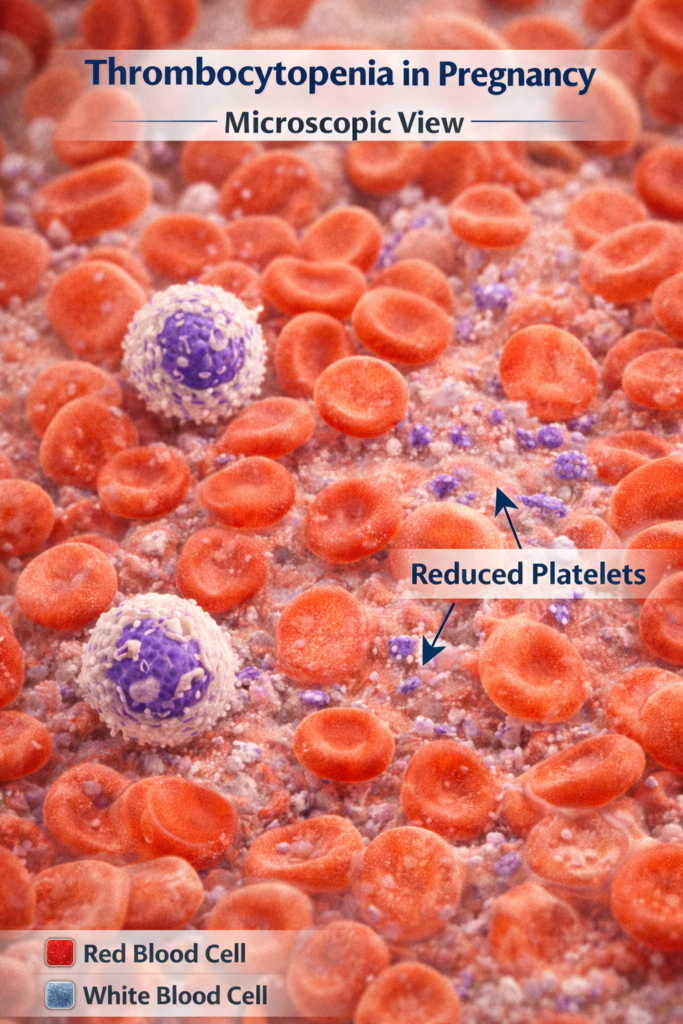
Thrombocytopenia in pregnancy is a condition where a pregnant woman has a lower than normal number of platelets in her blood. Platelets are tiny blood cells that help your blood clot properly when you are injured. When platelet levels drop too low, your body cannot control bleeding as effectively as it should.
A normal platelet count ranges from 150,000 to 400,000 platelets per microliter of blood. When this count falls below 150,000, the condition is called thrombocytopenia.
During pregnancy, the body goes through major changes in blood volume and circulation. Because of these natural changes, a mild drop in platelet count is actually quite common and is not always a reason for serious concern. However, understanding thrombocytopenia in pregnancy matters because while some causes are completely harmless, others can signal a more serious underlying condition that needs prompt medical attention.
2. How Common Is Thrombocytopenia in Pregnancy?
Thrombocytopenia in pregnancy is more common than most people realize. It affects approximately 7 to 12 percent of all pregnant women, making it the second most common blood disorder seen during pregnancy, right after anemia.
Around 70 to 80 percent of all cases are mild and fall under a category called gestational thrombocytopenia, which is harmless to both mother and baby. These mild cases typically resolve on their own after delivery without any treatment.
The condition can occur at any stage of pregnancy but is more commonly seen in the third trimester. Severe thrombocytopenia in pregnancy, where platelet counts drop below 100,000, occurs in only about 1 percent of pregnancies.
3. Causes of Thrombocytopenia in Pregnancy
There are several different causes of thrombocytopenia in pregnancy. Understanding the cause is essential because each type requires a very different approach to management.
Gestational Thrombocytopenia
This is by far the most common cause, accounting for 70 to 80 percent of all cases. It happens because pregnancy naturally increases blood volume, which dilutes the concentration of platelets in the bloodstream. It usually develops in the second or third trimester, is always mild, and platelet counts typically stay above 70,000. There is no increased risk of bleeding for the mother or baby, and it resolves completely after delivery.
Immune Thrombocytopenia (ITP)
ITP is an autoimmune condition where the body’s immune system mistakenly attacks and destroys its own platelets. It accounts for around 1 to 4 percent of thrombocytopenia in pregnancy cases. Unlike gestational thrombocytopenia, ITP can develop at any stage of pregnancy and may cause platelet counts to drop much lower sometimes below 10,000. Because the antibodies involved can cross the placenta, there is a small risk that the baby may also have low platelets at birth.
Preeclampsia and HELLP Syndrome
Preeclampsia is a serious pregnancy complication involving high blood pressure and organ damage. In some cases, it also causes thrombocytopenia in pregnancy. A more severe form called HELLP syndrome which stands for Hemolysis, Elevated Liver enzymes, and Low Platelet count is a life-threatening condition requiring immediate medical intervention. In a 2025 study of 151 women with thrombocytopenia in pregnancy, those with hypertensive disorders had the lowest newborn birth weights and higher rates of babies needing intensive care.
Other Causes
Less commonly, thrombocytopenia in pregnancy can result from:
- Vitamin B12 or folate deficiency
- Viral infections such as HIV or hepatitis
- Liver disease or systemic lupus erythematous (SLE)
- Anti-phospholipid syndrome
- Certain medications that interfere with platelet production
4. Signs and Symptoms
Many women with mild thrombocytopenia in pregnancy have absolutely no symptoms at all. The condition is often discovered during a routine prenatal blood test. However, as platelet counts drop lower, certain warning signs can appear.
Clinical Signs and Symptoms:
- Easy bruising bruises appearing with little or no injury
- Petechiae tiny red or purple spots on the skin that look like a rash
- Bleeding gums when brushing teeth
- Frequent or hard-to-stop nosebleeds
- Prolonged bleeding from small cuts
- Blood in urine or stools
- Heavy or unusual bleeding that is difficult to control
It is important to note that serious or spontaneous bleeding typically only occurs when platelet counts fall below 10,000 to 20,000. For counts between 20,000 and 100,000, bleeding usually only happens with surgical or invasive procedures rather than on its own.
If you notice any of the symptoms listed above during your pregnancy, do not ignore them. Contact your healthcare provider right away. Early detection of thrombocytopenia in pregnancy can prevent complications and keep both you and your baby safe.
5. Risks for Mother and Baby
The level of risk associated with thrombocytopenia in pregnancy depends largely on how low the platelet count drops and what is causing it.
For the Mother:
- In mild gestational thrombocytopenia, the risk is very low and no special precautions are needed
- If platelet counts fall significantly, there is an increased risk of excessive bleeding during labor and delivery
- A common concern is whether a woman with thrombocytopenia in pregnancy can safely receive an epidural. Most anesthesiologists consider epidurals safe when platelet counts are above 70,000 to 80,000, but this is always decided individually by the medical team
- In cases related to HELLP syndrome or severe preeclampsia, risks are much more serious and may require urgent early delivery
For the Baby:
- In gestational thrombocytopenia, the baby is not affected at all
- In ITP cases, maternal antibodies can cross the placenta and cause neonatal thrombocytopenia low platelets in the newborn
- The baby’s platelet count is checked right after birth and usually improves on its own within a few weeks
6. Diagnosis
Diagnosing thrombocytopenia in pregnancy is usually straightforward. It is most often identified through a Complete Blood Count (CBC), which is a standard blood test done during routine prenatal visits.
Once low platelet levels are found, your doctor will take steps to find the underlying cause:
- Medical history review asking about previous bleeding problems, autoimmune conditions, family history, and current medications
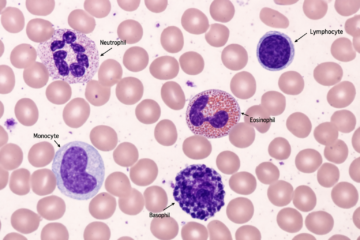
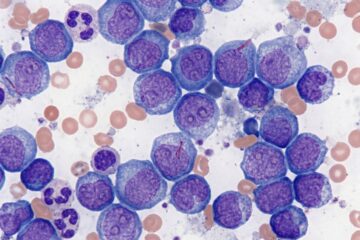
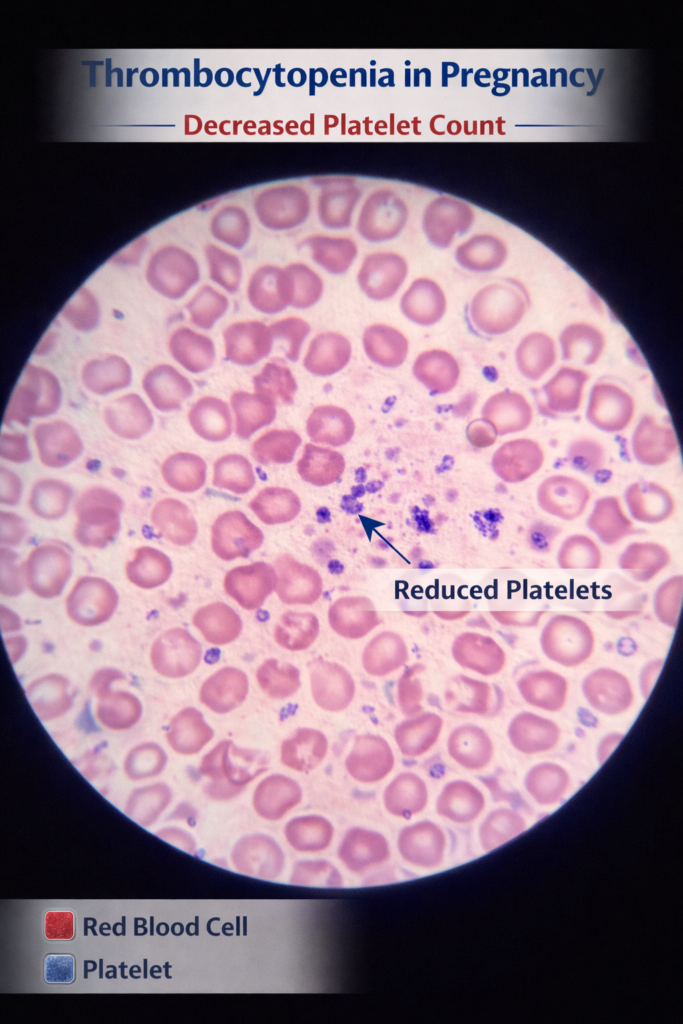
- Blood smear examination looking at blood cells under a microscope to check their shape and appearance
- Liver function tests checking for preeclampsia or HELLP syndrome
- Autoimmune antibody tests to identify ITP
- Viral infection screening testing for HIV, hepatitis, or other infections if relevant
- Vitamin deficiency testing checking folate and B12 levels
The timing of when thrombocytopenia in pregnancy appears also gives important clues. If it develops in the first or second trimester, ITP or a pre-existing condition is more likely. If it appears in the third trimester, gestational thrombocytopenia is the most probable cause.
According to the American College of Obstetricians and Gynecologists (ACOG), regular prenatal monitoring and timely investigation of low platelet counts are key components of safe pregnancy care.
7. Treatment Options
Treatment for thrombocytopenia in pregnancy depends entirely on the cause and how severe it is.
Gestational Thrombocytopenia
No treatment is needed. Your doctor will simply monitor your platelet count with regular blood tests. Platelet levels return to normal on their own within four to eight weeks after delivery.
Immune Thrombocytopenia (ITP)
Treatment is usually considered when platelet counts drop below 20,000 or when significant bleeding symptoms appear. The main options include:
- Corticosteroids (Prednisone) taken at 20 to 60 mg daily, they reduce the immune system’s attack on platelets and are the most common first-line treatment
- Intravenous Immunoglobulin (IVIG) given at 1 to 2 g/kg, IVIG works quickly to raise platelet counts and has an excellent safety profile during pregnancy. When combined with prednisone, it achieves the desired platelet response in around 80 percent of cases
- Second-line options in difficult or non-responsive cases, specialists may consider thrombopoietin receptor agonists or other immunosuppressants
Preeclampsia and HELLP Syndrome
These are medical emergencies requiring immediate hospital care. Treatment typically includes:
- Blood pressure medications
- Magnesium sulfate to prevent seizures
- Platelet transfusions in severe cases
- Early delivery of the baby when necessary to protect both mother and child
Nutritional Deficiencies
If thrombocytopenia in pregnancy is linked to a deficiency in folate or vitamin B12, appropriate dietary changes and supplementation are usually all that is needed to restore platelet counts.
For the latest treatment guidance, visit the Centers for Disease Control and Prevention (CDC) for regularly updated recommendations.
8. Delivery Planning
Safe delivery with thrombocytopenia in pregnancy requires careful planning and close teamwork between your obstetrician, hematologist, and anesthesiologist.
Target platelet counts for safe delivery:
- Vaginal delivery: platelet count of 50,000 or above is generally considered safe
- Cesarean delivery: platelet count of 50,000 or higher is recommended
- Epidural or spinal anesthesia: platelet count of 70,000 to 80,000 or above is typically required
Most women with mild thrombocytopenia in pregnancy can have a completely normal vaginal delivery. Cesarean delivery is not required solely because of a low platelet count unless there are other medical reasons. Your medical team will check your platelet count in the final weeks of pregnancy and adjust the birth plan accordingly to ensure everything goes as safely as possible.
Conclusion :
Thrombocytopenia in pregnancy can sound frightening when you first hear the words, but for the vast majority of women, it is a mild and completely manageable condition. The most important things you can do are attend all your prenatal appointments, get your routine blood tests done, and never ignore any unusual symptoms like unexplained bruising or bleeding.
Your healthcare team including your obstetrician, hematologist, and anesthesiologist, will work together to monitor your platelet count and create a birth plan that keeps you and your baby as safe as possible.
With the right care, proper monitoring, and early intervention when needed, most women with thrombocytopenia in pregnancy go on to have healthy, successful deliveries. You are not alone in this, and the medical community has extensive experience managing this condition safely.
Stay informed, stay connected with your care team, and trust that with the right support, a healthy outcome for both you and your baby is absolutely achievable.
Frequently Asked Questions
Is thrombocytopenia in pregnancy dangerous?
For most women, no. Mild gestational thrombocytopenia is the most common type and poses no danger to mother or baby. However, severe cases caused by ITP or HELLP syndrome carry real risks and need careful specialist management.
Can I have a normal delivery with thrombocytopenia in pregnancy?
Yes, in most cases. As long as platelet counts are at a safe level, a normal vaginal delivery is possible. Your medical team will assess your count close to your due date and plan accordingly.
Will my baby have low platelets too?
In gestational thrombocytopenia, no the baby is not affected. In ITP cases, the baby may be born with low platelets, but this is closely monitored and usually resolves on its own within a few weeks.
Does thrombocytopenia in pregnancy go away after delivery?
Gestational thrombocytopenia resolves completely within one to two months after delivery. ITP may persist after pregnancy but is manageable with ongoing specialist care.
Can I take supplements to help with my platelet count?
Never take supplements or medications without speaking to your doctor first. If a nutritional deficiency is contributing to your low platelet count, your doctor will recommend exactly what you need. Self-medicating during pregnancy can be harmful to both you and your baby.
When should I call my doctor immediately?
Contact your healthcare provider right away if you experience unexplained or excessive bruising, bleeding that will not stop, tiny red spots on your skin, severe headache, vision changes, or upper abdominal pain on the right side. These can be signs of a serious condition that needs urgent attention.
Disclaimer:
This content is for educational and public health awareness only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider for diagnosis, treatment, or prevention guidance.