Introduction
Rabies post exposure prophylaxis is not something you want to delay even for a single day. Rabies is almost always fatal once symptoms appear — but with the right treatment started quickly after exposure, it is completely preventable.
Every year, tens of thousands of people around the world begin rabies post exposure prophylaxis after being bitten, scratched, or licked by a potentially infected animal. When this treatment is given correctly and promptly, it stops the virus in its tracks — before it ever reaches the brain.
In this article, we cover what rabies post exposure prophylaxis involves, when you need it, the 5 essential steps of the treatment process, who is at highest risk, and what happens if treatment is delayed.
What Is Rabies Post Exposure Prophylaxis?
Rabies post-exposure prophylaxis – commonly abbreviated as PEP – is a series of preventive medical treatments given to a person after they have been potentially exposed to the rabies virus.
The rabies virus is a deadly pathogen that spreads through the saliva of infected animals, typically through bites. Once it enters the body, it travels slowly along nerve pathways toward the brain. During this travel period — which can last days to months depending on the location of the bite — the virus has not yet reached critical organs. This window is your opportunity to intervene.
Rabies post exposure prophylaxis works by introducing antibodies and triggering the immune system to fight the virus before it causes irreversible neurological damage.
According to the Centers for Disease Control and Prevention (CDC), PEP consists of three key components: thorough wound care, human rabies immune globulin (HRIG), and a four-dose rabies vaccine series.

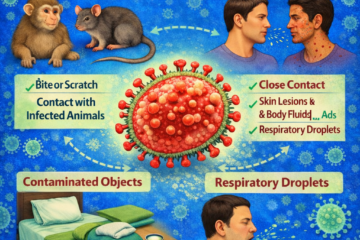
Which Animals Can Transmit Rabies?
Before understanding when rabies post exposure prophylaxis is needed, it helps to know which animals carry the highest risk.
- Dogs (especially in countries where canine rabies is endemic)
- Bats — considered one of the most common sources in many regions
- Raccoons, foxes, skunks, and jackals
- Cats in areas where vaccination rates are low
Lower-risk but still relevant animals:
- Cattle, horses, and goats can also carry rabies but bite humans less frequently
Animals that do not typically carry rabies:
- Small rodents such as mice, rats, squirrels, and hamsters
- Rabbits
- Birds, reptiles, fish, and insects
If you are bitten or scratched by an animal you cannot identify, or by a bat that has been in the same room while you were sleeping, it is important to treat it as a possible rabies exposure and seek medical attention immediately.
5 Urgent Steps of Rabies Post Exposure Prophylaxis
Step 1 — Wash the Wound Immediately
The very first thing you should do after a potential rabies exposure is wash the wound thoroughly with soap and running water for a minimum of 15 minutes.
This is not just basic first aid — it is a medically critical step in rabies post exposure prophylaxis. Studies in animal models have shown that thorough wound washing alone can significantly reduce the likelihood of viral transmission. The physical flushing and detergent action of soap helps remove viral particles from the wound site.
After washing with soap and water, apply a disinfectant such as povidone-iodine solution or 70% alcohol to further reduce the risk of both rabies and bacterial infection.
Do not close or suture the wound without medical guidance. In some cases, early wound closure can increase infection risk.
Step 2 — Seek Medical Care Without Delay
After washing the wound, go to a doctor, emergency room, or rabies treatment center as quickly as possible — ideally within hours of the exposure.
Do not wait to see if symptoms develop. By the time rabies symptoms appear, the virus has already reached the brain. At that stage, there is no effective treatment, and death is almost certain.
A medical professional will assess the nature of the exposure, the animal involved, and your vaccination history to determine the appropriate rabies post exposure prophylaxis protocol.
Step 3 — Receive Human Rabies Immune Globulin
Human rabies immune globulin — or HRIG — is the first active medical component of rabies post exposure prophylaxis.
HRIG contains pre-formed antibodies against the rabies virus. These antibodies act immediately, providing short-term protection while the body’s own immune system begins building a response to the vaccine.
HRIG is only given to people who have never previously been vaccinated against rabies. It is administered once — at the start of the PEP course — and is injected as much as possible directly into and around the wound site.
A critical rule highlighted by the CDC is that HRIG must never be administered in the same syringe or the same anatomical site as the first rabies vaccine dose — as this can interfere with vaccine effectiveness.
Step 4 — Complete the Full Rabies Vaccine Series
The rabies vaccine is the second and most important medical component of rabies post exposure prophylaxis. For people who have never been vaccinated against rabies before, a four-dose vaccine series is given on the following schedule:
- Day 0 — First dose given on the same day as HRIG
- Day 3 — Second dose
- Day 7 — Third dose
- Day 14 — Fourth and final dose
These vaccines are typically given as an injection into the upper arm (deltoid muscle) in adults, or into the outer thigh in young children. They should never be administered in the buttocks, as absorption is less reliable.
Each dose trains the immune system to recognize and attack the rabies virus. Together, the four doses build lasting protection that overwhelms the virus before it can progress.
For people who have previously been vaccinated against rabies: The protocol is different. HRIG is not needed. Only two vaccine doses are required — one on Day 0 and one on Day 3.
Step 5 — Follow Up and Do Not Miss Any Doses
Completing the full course of rabies post-exposure prophylaxis is essential. Missing a dose or delaying the schedule significantly reduces the treatment’s effectiveness.
After your final vaccine dose, your doctor may order a blood test to check your rabies antibody levels — particularly if you are immunocompromised, elderly, or taking medications that affect immune function.
People with weakened immune systems may require additional monitoring and potentially more doses, as their bodies may not respond to the vaccine as strongly as healthy individuals.
Who Needs Rabies Post Exposure Prophylaxis?
Not every animal bite requires PEP. However, it should always be considered a serious possibility. The following situations typically call for immediate rabies post exposure prophylaxis evaluation:
- A bite, scratch, or wound from a bat — even if you did not feel a bite (e.g., waking up to find a bat in your room)
- A bite or deep scratch from a dog, cat, or wild animal in a country or region where rabies is common
- Contact with saliva from a potentially rabid animal on broken skin or mucous membranes
- A bite from any animal showing unusual behavior — aggression, paralysis, excessive drooling, or disorientation
- Any situation where the animal cannot be observed or tested for rabies
If you are unsure, always consult a healthcare professional right away. The risk of not treating a true rabies exposure is death. The risk of unnecessarily completing PEP is minimal by comparison.
What Happens If Rabies Post Exposure Prophylaxis Is Delayed or Skipped?
This is a crucial point. Once rabies symptoms develop, the disease is almost universally fatal. No effective treatment exists at that stage.
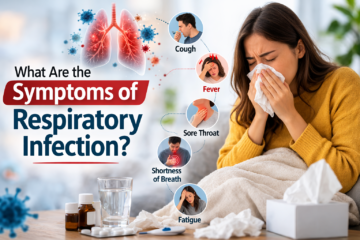
Rabies symptoms typically begin with flu-like signs — fever, headache, and fatigue — followed by neurological symptoms including confusion, agitation, hallucinations, hydrophobia (fear of water), and eventually paralysis and coma. Death usually occurs within days of symptom onset.
Globally, rabies kills an estimated 59,000 people each year — the vast majority in Asia and Africa, where access to PEP is limited or delayed.
This is why access to timely rabies post exposure prophylaxis is considered a public health priority. Healthcare guidelines from the Minnesota Department of Health and WHO-aligned national guidelines emphasize that the decision to start PEP should never be delayed waiting for lab confirmation.
Special Considerations
Immunocompromised individuals People with HIV, those on chemotherapy, or individuals taking immunosuppressant medications may not respond adequately to the standard PEP schedule. Additional doses and antibody titer testing are often recommended.
Pregnancy Pregnancy is not a reason to withhold rabies post exposure prophylaxis. The risk of untreated rabies to both mother and fetus far outweighs any theoretical concern about the vaccine.
Children Children are at higher risk of rabies exposure due to their interaction with animals and inability to always report bites. The PEP protocol is the same for children, with vaccine injected into the outer thigh in very young patients.
Travelers to rabies-endemic regions People traveling to countries in Asia, Africa, or Latin America where canine rabies is widespread should consider pre-exposure prophylaxis (PrEP) before their trip. PrEP does not eliminate the need for PEP after exposure, but it simplifies the treatment course and removes the need for HRIG.
Conclusion
Rabies post exposure prophylaxis is one of the most effective life-saving treatments in modern medicine — but only when it is used promptly and correctly. Every hour counts after a potential rabies exposure.
Wash the wound immediately. Seek medical care the same day. Complete the full vaccine course without interruption. These are not optional steps — they are the actions that stand between life and an almost certainly fatal disease.
If you or someone you know has been bitten or scratched by an animal in circumstances that raise concern, do not wait. Go to a healthcare provider now. Rabies post exposure prophylaxis works — but only when you act fast enough.
Frequently Asked Questions
How soon after exposure should PEP be started?
PEP should begin as soon as possible, ideally within 24 hours of exposure. Every hour of delay increases the risk of the virus reaching the brain via peripheral nerves. However, PEP can still be effective days or even weeks after exposure — it should never be withheld regardless of delay, as the incubation period may provide a window for prevention.
What are the PEP vaccine schedules?
There are several WHO-approved schedules. The most widely used are shown in the Quick Reference section below. For immunocompromised individuals, an additional dose on Day 28 (Zagreb) or Day 28 (Essen) is recommended. Intramuscular (IM) or intradermal (ID) routes may be used depending on the vaccine type and local protocol.
What is Rabies Immunoglobulin (RIG) and who needs it?
RIG provides immediate passive immunity while the vaccine takes 7–14 days to generate an active immune response. It is indicated for:
- Previously unvaccinated individuals with Category III exposure
- Severely immunocompromised individuals, regardless of prior vaccination
RIG is infiltrated into and around the wound on Day 0. Any remaining volume may be given IM at a distant site. It should not be given after Day 7 (when active immunity begins). Two types exist: Human RIG (HRIG) — preferred — and Equine RIG (ERIG) — purified.
How should a rabies-exposure wound be treated at home?
First aid wound care is critical and can significantly reduce the viral load:
- Wash immediately with soap and water for at least 15 minutes
- Apply a virucidal agent: povidone-iodine, 70% ethanol, or alcohol
- Avoid suturing the wound immediately — delay closure to reduce risk of viral spread
- If suturing is necessary, infiltrate RIG into the wound first
- Ensure tetanus prophylaxis and antibiotic coverage for secondary infection as clinically indicated
This step alone can prevent infection even before reaching a clinic.
Is PEP 100% effective if given correctly?
Yes — when administered promptly and correctly, PEP is virtually 100% effective. PEP failures are rare and typically occur due to:
- Delayed initiation of treatment
- Inadequate wound washing
- Failure to administer RIG when indicated (Category III)
- Incorrect injection technique or vaccine storage (cold chain failure)
- Incomplete vaccine course
Can PEP be given during pregnancy or in children?
Pregnancy is not a contraindication to PEP. Because rabies is almost universally fatal, the risk of not treating far outweighs any theoretical risk from vaccination. Modern cell-culture and purified chick embryo cell vaccines are safe in pregnancy. Similarly, PEP is indicated in children of all ages using the same vaccine schedule (weight-adjusted RIG dose in children).