⚡ Key Takeaways
- The troponin blood test measures proteins released into the bloodstream when heart muscle cells are injured.
- Two forms, troponin I and troponin T, are used in most hospital laboratories for cardiac risk assessment.
- High-sensitivity troponin assays can detect injury hours earlier than older-generation tests.
- Not every troponin rise points to a heart attack; kidney disease, sepsis, and intense exertion can also raise levels.
- Doctors usually repeat the troponin blood test over a few hours to track the pattern, not just a single number.
- A rising or falling trend carries more diagnostic weight than one isolated reading.
- Rapid 0/1-hour and 0/3-hour protocols now allow emergency departments to rule a heart attack in or out faster than ever.
1. Introduction to the Troponin Blood Test
When someone arrives at an emergency room with chest pain, the troponin blood test often becomes the single most decisive piece of evidence a physician relies on. It can confirm a heart attack within hours, or it can rule one out and send a worried patient home with reassurance.
This article walks through what the troponin blood test actually measures, how results are read, what else besides a heart attack can push the numbers up, and why this small vial of blood carries such enormous clinical weight in modern cardiology.
2. What Does the Troponin Blood Test Measure?
Troponin is a protein complex found inside heart muscle cells, where it helps regulate the contraction of cardiac fibers. Under normal conditions, almost none of it escapes into the bloodstream. The moment heart tissue becomes damaged or stressed, troponin leaks out of the injured cells and into circulation, where a blood draw can pick it up.
Because the molecule is found almost exclusively in heart tissue, the troponin blood test is considered far more specific for cardiac injury than older markers such as creatine kinase.
3. Types of Troponin Assays
3.1 Troponin I and Troponin T
Laboratories typically test for one of two subunits: cardiac troponin I (cTnI) or cardiac troponin T (cTnT). Both originate from heart muscle and are clinically interchangeable in most settings, though the specific cutoff values differ between manufacturers and assay platforms.
3.2 Conventional vs. High-Sensitivity Assays
Older conventional assays could only detect troponin once levels climbed fairly high, sometimes missing injury in its earliest hours. Newer high-sensitivity troponin (hs-cTn) assays can detect concentrations in the low picogram range, allowing clinicians to spot heart damage sooner and track subtle changes over time.
4. Why the Troponin Blood Test Matters Clinically
- It confirms or excludes acute myocardial infarction within a short, defined time window.
- It helps separate cardiac chest pain from non-cardiac causes such as muscle strain or acid reflux.
- It carries strong prognostic value, since higher peak levels are linked with greater heart muscle damage.
- It guides urgent treatment decisions, including whether a patient needs immediate catheterization.
5. How the Test Is Performed
A standard venous blood sample is drawn, usually from a vein in the arm, and sent to the laboratory or run on a point-of-care analyzer. No special fasting or preparation is generally required. In suspected heart attack cases, the sample is typically repeated at set intervals — often at presentation, then again one to three hours later — rather than relying on a single draw.
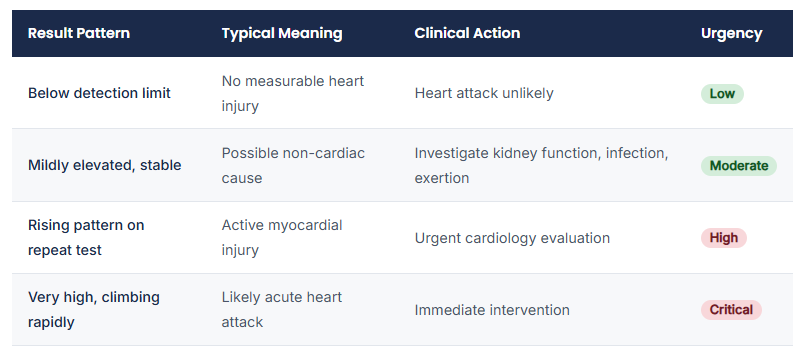
6. Reference Ranges and Interpreting Results
Exact cutoff values vary by laboratory and assay, so results should always be interpreted alongside the reference range printed on the lab report. As a general principle:
7. Causes of Elevated Troponin Beyond a Heart Attack
A raised troponin blood test result does not automatically mean a heart attack has occurred. Several other conditions can push levels upward:
- Chronic kidney disease, which slows the clearance of troponin from the blood
- Severe infections or sepsis, which place added strain on the heart
- Pulmonary embolism or other causes of strain on the right side of the heart
- Myocarditis, an inflammation of the heart muscle itself
- Extremely intense or prolonged physical exertion, such as marathon running
- Heart failure with ongoing muscle strain
This is why clinicians never read a troponin blood test in isolation. The full clinical picture — symptoms, ECG findings, and patient history — always shapes the final interpretation.
 Clinical Alert: Trend MatteNumberrs More Than a Single
Clinical Alert: Trend MatteNumberrs More Than a Single
A lone troponin reading rarely tells the whole story. Guidelines from major cardiology societies emphasize watching how the value changes between two or more draws, since a clear rise or fall pattern is far more diagnostic than any single isolated result.
8. Diagnostic Algorithms: Serial Testing and Rapid Protocols
Many emergency departments now follow structured rapid protocols built around high-sensitivity troponin testing:
- 0/1-hour protocol: a baseline sample followed by a second draw just one hour later, allowing very fast rule-out or rule-in decisions.
- 0/3-hour protocol: a slightly longer window used when the first result falls into an intermediate, less clear-cut zone.
- Single-sample rule-out: in select low-risk patients, an extremely low first reading combined with a reassuring symptom picture may be enough to avoid further testing.
According to guidance summarized by the American Heart Association, these accelerated pathways have meaningfully shortened emergency department stays without compromising patient safety.
9. Risk Stratification and Prognostic Value
Beyond diagnosing an active heart attack, the troponin blood test also carries long-term prognostic meaning. Patients with higher peak troponin levels generally face a greater risk of future cardiac events, reduced heart pumping function, and higher short-term mortality compared with those whose levels stay low or normal.
10. Limitations and Possible False Results
- False elevation: kidney impairment, certain antibodies, or assay interference can occasionally raise readings without true heart injury.
- Delayed rise: very early after symptom onset, troponin may still be within normal range even if injury has begun, which is why repeat testing matters.
- Assay variability: different manufacturers use different cutoffs, so results from separate laboratories are not always directly comparable.
11. Troponin Versus Other Cardiac Biomarkers
Older markers such as creatine kinase-MB (CK-MB) and myoglobin were once standard tools for detecting heart injury. Troponin has largely replaced them because it remains elevated for a longer window — often five to fourteen days — and offers superior specificity for heart muscle damage, reducing the chance of a misleading result from unrelated muscle injury.
12. Preparing for the Test and What to Expect
No fasting, special diet, or medication adjustment is typically needed before a troponin blood test. The procedure itself is a routine blood draw, taking only a few minutes, with mild and temporary discomfort at the needle site. Results from high-sensitivity assays are often available within an hour, which is part of why the test has become central to fast-moving emergency care.
13. Recent Advances in Troponin Testing
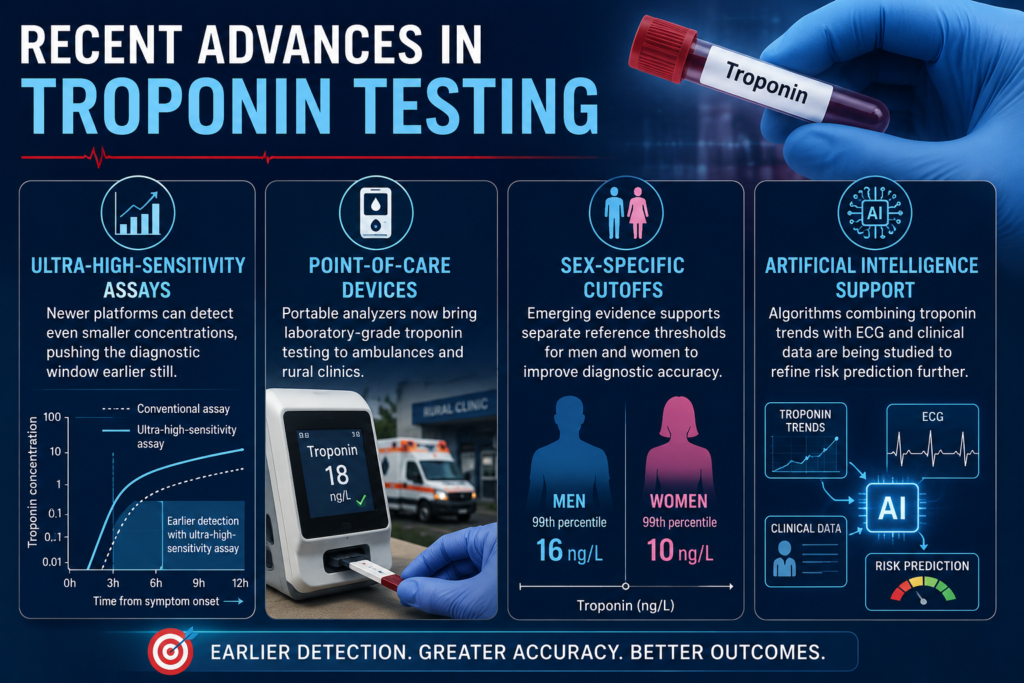
- Ultra-high-sensitivity assays: newer platforms can detect even smaller concentrations, pushing the diagnostic window earlier still.
- Point-of-care devices: portable analyzers now bring laboratory-grade troponin testing to ambulances and rural clinics.
- Sex-specific cutoffs: emerging evidence supports separate reference thresholds for men and women to improve diagnostic accuracy.
- Artificial intelligence support: algorithms combining troponin trends with ECG and clinical data are being studied to refine risk prediction further.
14. Future Perspectives in Cardiac Biomarker Testing
Research continues to push the boundaries of what the troponin blood test can reveal. Investigators are exploring how combining troponin with other emerging biomarkers might better distinguish chronic, low-grade heart strain from a true acute event. Wearable sensor technology and home-based micro-sampling devices are also being studied as a way to monitor at-risk patients outside the hospital setting.
15. Conclusion and Key Takeaways
The troponin blood test has transformed how clinicians evaluate chest pain and suspected heart injury, offering a fast, sensitive, and highly specific window into the health of the heart muscle. Understanding what drives a result up, how trends are interpreted, and when urgent action is required helps both healthcare professionals and patients make sense of this small but powerful test.
A single number rarely tells the full story, but paired with clinical judgment, the troponin blood test remains one of the most valuable tools in modern cardiac care.
Clinical Relevance for Laboratory and Healthcare Professionals
Always interpret troponin results against the assay-specific reference range, not a generic universal cutoff.
Document the exact timing of symptom onset relative to each blood draw, since this affects interpretation.
Consider non-cardiac causes of elevation in patients with kidney disease, sepsis, or recent extreme exertion.
Use serial sampling and delta-change criteria rather than relying on one isolated value.
Correlate every result with the patient’s symptoms, ECG, and overall clinical context before making treatment decisions.
Frequently Asked Questions (FAQ)
What does a high troponin blood test result mean?
A high result suggests injury to heart muscle cells, most commonly from a heart attack, though other conditions such as kidney disease, sepsis, or myocarditis can also raise the level.
How quickly do troponin levels rise after a heart attack?
Levels typically begin rising within two to three hours of symptom onset, peak around twelve to twenty-four hours later, and can remain detectable for several days afterward.
Can troponin be elevated without a heart attack?
Yes. Kidney failure, severe infection, pulmonary embolism, heart failure, and intense physical exertion can all raise troponin without an actual heart attack occurring.
Why is the troponin blood test repeated more than once?
A single reading can miss early injury or be misleading on its own. Repeating the test allows doctors to see whether the level is rising, falling, or staying flat, which is far more informative.
Is the troponin blood test painful?
It involves a standard blood draw from a vein, similar to any routine blood test. Discomfort is usually mild and brief.
What is the difference between troponin I and troponin T?
Both are subunits of the same troponin protein complex released from injured heart muscle. They are generally considered clinically equivalent, though specific cutoff values differ depending on the assay used.