📋 Table of Contents
- What Is the Mechanism of Antibiotic Resistance?
- Classification of Antibiotic Resistance
- Types of Resistance Mechanisms (7 Major Pathways)
- How Resistance Spreads: Horizontal Gene Transfer
- Why Antibiotic Resistance Is Accelerating
- Strategies to Combat Antibiotic Resistance
- Summary Table
- Frequently Asked Questions
Key takeaway: The mechanism of antibiotic resistance is not a single event — it is a collection of brilliant, constantly evolving survival strategies that bacteria use to neutralize even our most powerful drugs. Understanding these mechanisms is foundational to clinical microbiology, diagnostic laboratory practice, infection control, and global public health policy.
Introduction:
Antibiotic resistance stands as one of the most pressing threats to modern medicine. Every year, drug-resistant bacterial infections claim over a million lives worldwide — and the numbers keep climbing. What makes this especially alarming is that we are losing ground faster than we are developing new treatments.
For medical laboratory technology (MLT) students, clinicians, and healthcare professionals, understanding the mechanism of antibiotic resistance is not optional — it is essential. From interpreting antibiogram reports to guiding empirical therapy decisions, the principles covered in this article apply directly to real-world clinical practice.
What Is the Mechanism of Antibiotic Resistance?
In simple terms, the mechanism of antibiotic resistance refers to the specific biological strategies bacteria use to survive exposure to antibiotics. These are not random accidents — they are the product of evolutionary pressure, genetic adaptability, and millions of years of microbial survival instinct.
Antibiotics work by targeting very specific structures or processes inside a bacterial cell — the cell wall, protein synthesis ribosomes, DNA gyrase, or folic acid synthesis pathways. Resistant bacteria find ways to destroy, avoid, modify, or bypass these attacks entirely.
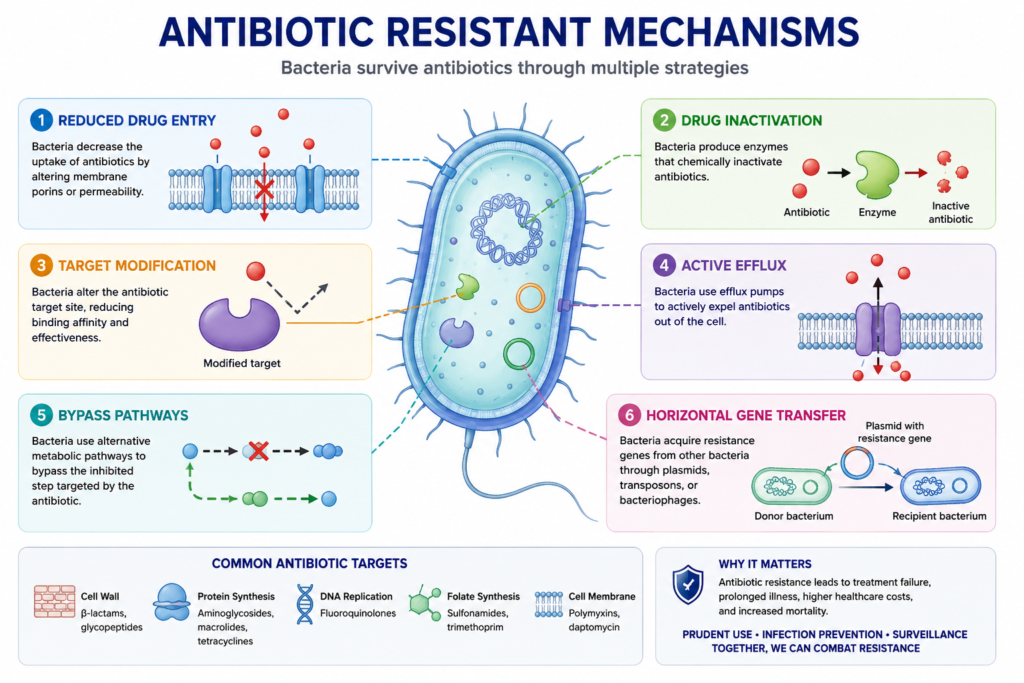
There are four broad categories of resistance strategies:
⚗️ Enzymatic inactivation — bacteria produce enzymes that chemically destroy or modify the antibiotic before it can act
🔧 Modification of the drug target — the antibiotic’s binding site on the bacterium is altered so the drug can no longer attach
🚪 Reduced uptake or increased efflux — either less antibiotic enters the cell, or it is actively pumped back out
🔄 Bypass of the targeted pathway — bacteria find an alternative metabolic route that skips the blocked step entirely
All four lead to the same result: the antibiotic fails to kill the bacteria at therapeutic concentrations.
Classification of Antibiotic Resistance
The classification of antibiotic resistance helps researchers and clinicians understand both the origin and the operational mechanism of resistance — two different but equally important perspectives.
A. Classification by Origin
Natural / Innate Resistance
Some bacteria are inherently resistant to certain antibiotics as part of their normal biology — before any drug exposure ever occurs. For example, gram-negative bacteria possess an outer membrane (lipopolysaccharide layer) that naturally blocks many antibiotics, including vancomycin. Pseudomonas aeruginosa has multiple intrinsic resistance mechanisms due to its low outer membrane permeability and constitutively expressed efflux pumps.
Developed / Adaptive Resistance
This occurs when bacteria that were previously susceptible to an antibiotic develop resistance over time. It happens through spontaneous chromosomal mutations (e.g., changes in drug-binding sites) or through horizontal gene transfer — acquiring pre-built resistance genes from neighboring bacteria via plasmids or other mobile genetic elements.
B. Classification by Mechanism
This groups resistance by how it works at the molecular level — enzymatic destruction, target alteration, reduced drug accumulation, or pathway bypass. The full mechanistic breakdown follows in the next section.
💡 Lab Relevance:
In the clinical microbiology laboratory, distinguishing between intrinsic and acquired resistance is critical when reading antibiograms and applying CLSI/EUCAST breakpoints. A reported resistance pattern that matches known intrinsic resistance does not require investigation — but an unexpected acquired resistance in a typically susceptible species is a red flag requiring further characterization.
Types of Antibiotic Resistance Mechanisms
Below are the seven most clinically significant mechanisms of antibiotic resistance, each explained with its molecular basis, clinical examples, and diagnostic relevance.
Enzymatic Inactivation
Bacteria produce enzymes that chemically modify or destroy the antibiotic before it reaches its target. This is the most common and clinically important mechanism worldwide. The prime example is beta-lactamase production — an enzyme that breaks the beta-lactam ring in penicillins and cephalosporins, rendering them inactive. Extended-spectrum beta-lactamases (ESBLs) and carbapenemases (e.g., NDM-1, KPC) represent especially dangerous variants. Aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases, nucleotidyltransferases) are another important example.
Target Modification
Bacteria alter the structure of the antibiotic’s binding site so the drug can no longer attach effectively. MRSA (Methicillin-resistant Staphylococcus aureus) is the textbook example: it produces a modified penicillin-binding protein (PBP2a, encoded by the mecA gene) with very low affinity for beta-lactams. Similarly, Streptococcus pneumoniae develops penicillin resistance through altered PBPs, and rifampicin resistance arises from mutations in the rpoB gene encoding RNA polymerase.
Efflux Pumps
Efflux pumps are membrane-embedded protein transporters that actively eject antibiotics from the bacterial cell before they can reach effective concentrations. What makes this particularly dangerous is that many efflux pumps are multidrug efflux systems — they simultaneously expel multiple antibiotic classes, resulting in multidrug resistance (MDR) in a single genetic step. Pseudomonas aeruginosa‘s MexAB-OprM and MexCD-OprJ pump systems are well-known clinical examples. The AcrAB-TolC system in Enterobacteriaceae is another major concern.
Reduced Permeability
Gram-negative bacteria have outer membrane protein channels called porins (e.g., OmpC, OmpF) that serve as entry gates for hydrophilic antibiotics such as carbapenems. Bacteria can develop resistance by reducing porin expression, producing mutant porins, or switching to smaller-channel isoforms. When porin loss combines with ESBL or carbapenemase production, the result is pan-drug-resistant (PDR) organisms — bacteria for which virtually no antibiotic works.
Bypass Mechanisms
Some bacteria develop or acquire alternative metabolic pathways that circumvent the drug target entirely. Sulfonamides block dihydropteroate synthase, an enzyme bacteria need for de novo folate synthesis. Resistant bacteria simply acquire the ability to import preformed folate from the surrounding environment, bypassing the blocked pathway altogether. Vancomycin-resistant enterococci (VRE) employ a related strategy, producing modified cell wall precursors (D-Ala-D-Lac instead of D-Ala-D-Ala) that vancomycin cannot bind.
Target Protection
Rather than permanently altering the drug target, some bacteria produce protection proteins that physically shield the target from the antibiotic, or displace the drug after it binds. Tetracycline resistance proteins (e.g., Tet(M), Tet(O)) protect the 30S ribosomal subunit from tetracycline binding. Fluoroquinolone resistance mediated by Qnr proteins protects DNA gyrase and topoisomerase IV from quinolone action — a mechanism spread by plasmids globally.
Biofilm Formation
Biofilms are structured, surface-attached bacterial communities embedded within a self-produced extracellular matrix of polysaccharides, proteins, and extracellular DNA. This matrix creates a physical barrier to antibiotic penetration, but the resistance is not only physical — bacteria inside biofilms also exhibit drastically altered gene expression, reduced metabolic rates (making them “tolerant” to antibiotics that target actively dividing cells), and efflux pump upregulation. Bacteria inside biofilms can be 100–1,000 times more resistant than their planktonic counterparts. Biofilms form readily on catheters, prosthetic joints, cardiac implants, and wound surfaces.
⚠️ Critical Clinical Note: Combination Resistance
In practice, resistant bacteria rarely rely on just one mechanism. Organisms like carbapenem-resistant Klebsiella pneumoniae (CRKP) often combine carbapenemase production + porin loss + efflux pump overexpression simultaneously. This synergistic combination is what drives pan-drug resistance and makes some infections virtually untreatable with current antibiotics.
How Resistance Spreads: Horizontal Gene Transfer (HGT)
The mechanism of antibiotic resistance becomes truly alarming when we consider how quickly resistance genes can spread — not just within a species, but across entirely different bacterial genera. This happens through horizontal gene transfer (HGT), which allows bacteria to share genetic material during their own lifetimes (unlike vertical gene transfer, which passes genes only to daughter cells during reproduction).
Bacteria establish direct cell-to-cell contact through a structure called a pilus and transfer resistance-encodingplasmids(extrachromosomal circular DNA). A single resistant bacterium can pass its plasmid to thousands of susceptible neighbours in a short time. Conjugative plasmids can carry multiple resistance genes simultaneously, enabling rapid spread of multidrug resistance. ESBL genes, carbapenemase genes (blaNDM, blaKPC, blaOXA-48), and colistin resistance genes (mcr-1) are all plasmid-borne.
Transformation — Uptake of Environmental DNA
Some bacteria are naturally “competent” — they can actively take up and incorporate naked DNA fragments from their environment, including genetic material released from dead resistant bacteria. Streptococcus pneumoniae acquires penicillin resistance through transformation, picking up altered PBP genes from closely related streptococci.
Transduction — Bacteriophage-Mediated Transfer
Bacteriophages (viruses that infect bacteria) can accidentally package bacterial DNA — including resistance genes — and transfer it to the next bacterium they infect. This mechanism operates at smaller scales than conjugation but can still contribute meaningfully to resistance gene mobilisation in environments like hospital intensive care units and wastewater treatment plants.
🧫 Mobile Genetic Elements (MGEs)
Resistance genes are often located on mobile genetic elements — plasmids, transposons, integrons, and genomic islands — that are specifically designed for movement between DNA molecules and between bacterial cells. Integrons are particularly important: they can capture and express multiple resistance gene cassettes, acting as natural gene-collection platforms within a single bacterial cell.
Why Is Antibiotic Resistance Getting Worse?
The rise of resistance is not simply a biological inevitability — it is being accelerated by human behaviour, systemic failures, and economic disincentives. Here are the major drivers:
💊 Antibiotic Overuse in Medicine
Antibiotics are frequently prescribed for viral respiratory infections where they have absolutely no therapeutic effect. Every unnecessary antibiotic course exerts selective pressure on commensal bacteria, promoting resistance gene acquisition and spread. In many low- and middle-income countries — including parts of South Asia — antibiotics are available over the counter without prescription, dramatically worsening the problem.
🐄 Massive Agricultural Use
More than 70% of medically important antibiotics sold globally are used in livestock farming — primarily for growth promotion and disease prevention in crowded conditions. This creates enormous environmental reservoirs of resistance genes in animal intestines, soil, water, and the food supply chain. The mcr-1 colistin resistance gene, for example, originated in livestock settings before spreading to human pathogens globally.
🏥 Poor Infection Prevention & Control (IPC)
Healthcare-associated infections (HAIs) caused by multidrug-resistant organisms spread readily in hospitals with inadequate hand hygiene, environmental cleaning, and isolation practices. Shared equipment, over-crowded wards, and insufficient microbiological surveillance all contribute to in-hospital amplification and patient-to-patient transmission of resistant strains.
 Empty Antibiotic Pipeline
Empty Antibiotic Pipeline
Pharmaceutical companies have largely abandoned antibiotic development because new antibiotics are not commercially profitable — they are used sparingly, for short durations, and often for the sickest patients. No truly novel antibiotic class has been introduced into clinical practice since the 1980s. The pipeline for gram-negative pathogens — the most dangerous drug-resistant organisms — is critically thin.
According to the World Health Organization (WHO), antimicrobial resistance is among the most urgent global health threats, with resistant infections already claiming over 1.27 million lives annually as a direct cause. The WHO’s Priority Pathogen List identifies critical-priority pathogens — including carbapenem-resistant Acinetobacter baumannii, Pseudomonas aeruginosa, and carbapenem-resistant Enterobacteriaceae — as the most urgent targets for new drug development.
Strategies to Combat Antibiotic Resistance
Despite the scale of the challenge, there are proven, evidence-based interventions that can slow resistance spread, preserve existing antibiotics, and develop new solutions.
📋 Antibiotic Stewardship Programs (ASPs)
Structured, multidisciplinary programs that promote prescribing the right antibiotic, at the right dose, for the right duration, via the right route. ASPs combine prospective audit with feedback, formulary restriction, de-escalation protocols, and pharmacist-physician collaboration. Studies consistently show ASPs reduce resistance rates, lower C. difficile infection rates, shorten hospital stays, and reduce antibiotic costs.
🔭 Rapid Molecular Diagnostic Testing
Traditional culture and sensitivity results take 48–72 hours. Rapid PCR-based diagnostics (e.g., BioFire FilmArray, Xpert MTB/RIF) can identify both the pathogen and key resistance genes within hours, enabling targeted therapy rather than broad-spectrum empirical treatment and significantly reducing antibiotic overuse.
💉 Vaccination Programmes
Every vaccine-preventable infection averted is an antibiotic course that never needs to be prescribed. Pneumococcal, meningococcal, Hib, and typhoid vaccines directly reduce the burden of bacterial infections requiring antibiotic therapy. The broad rollout of pneumococcal conjugate vaccines (PCV) has measurably reduced penicillin-resistant S. pneumoniae carriage rates in vaccinated populations.
🧪 Novel Therapeutic Approaches
Research is actively exploring alternatives to conventional antibiotics:
phage therapy (using bacteriophage viruses to kill specific bacteria),
antimicrobial peptides,
anti-virulence strategies (targeting bacterial toxins or biofilm formation without killing the bacteria),
CRISPR-Cas antimicrobials, andmicrobiome-protective therapies. While most are still in pre-clinical or early clinical stages, they represent the future of antimicrobial medicine.
🌐 International Surveillance Networks
Real-time resistance data guides clinical guidelines, drug approvals, and outbreak responses. The CDC’s National Antimicrobial Resistance Monitoring System (NARMS) tracks resistance across food animals, retail meat, and humans. The WHO Global Antimicrobial Resistance and Use Surveillance System (GLASS) coordinates national surveillance across 70+ countries, including regional networks in South Asia.
📢 Public Education & Awareness
Antibiotic resistance is partly driven by patient demand for antibiotics during viral illness, self-medication, and failure to complete full antibiotic courses. Community education campaigns — especially relevant in Nepal and South Asia where over-the-counter antibiotic access is widespread — can meaningfully shift these behaviours and reduce selective pressure at the population level.
Summary Table: Mechanisms of Antibiotic Resistance at a Glance
| Mechanism | How It Works | Key Examples | Clinical Significance |
|---|---|---|---|
| Enzymatic Inactivation | Enzymes chemically destroy or modify the antibiotic | Beta-lactamase, ESBL, NDM-1, KPC | CRITICAL |
| Target Modification | Drug-binding site is structurally altered | MRSA (PBP2a), VRE (D-Ala-D-Lac), rifampicin-R TB | CRITICAL |
| Efflux Pumps | Antibiotic is actively expelled from the cell | P. aeruginosa MexAB-OprM; AcrAB-TolC in Enterobacteriaceae | HIGH |
| Reduced Permeability | Fewer or mutant porins reduce drug entry | Carbapenem resistance in Klebsiella, E. coli | HIGH |
| Bypass Mechanisms | Alternative pathway circumvents blocked target | Sulfonamide resistance (folate import); VRE | MODERATE |
| Target Protection | Protective proteins shield target from drug | Tet(M) ribosome protection; Qnr proteins | MODERATE |
| Biofilm Formation | Physical matrix blocks antibiotic penetration; altered metabolism | Catheter-related infections, prosthetic joint infections | HIGH |
Frequently Asked Questions
What is the mechanism of antibiotic resistance in simple terms?
In simple terms, antibiotic resistance is what happens when bacteria develop the ability to survive drug concentrations that would normally kill them. They achieve this through several strategies: destroying the antibiotic with enzymes, changing the shape of the drug’s target so it can’t bind, pumping the drug out before it works, or finding an entirely different metabolic pathway that doesn’t need the blocked step. These strategies can arise from genetic mutations or be acquired from other bacteria.
What is the difference between intrinsic and acquired antibiotic resistance?
Intrinsic resistance is a natural, inherent feature of a bacterial species — it exists before any antibiotic exposure. For example, all gram-negative bacteria are intrinsically resistant to vancomycin because the drug cannot penetrate their outer membrane. Acquired resistance, on the other hand, develops in bacteria that were originally susceptible. It arises through random chromosomal mutations or through horizontal gene transfer — picking up ready-made resistance genes from other bacteria via plasmids or other mobile genetic elements.
How do efflux pumps cause antibiotic resistance?
Efflux pumps are specialized protein transporters embedded in the bacterial cell membrane. They work like molecular bouncers — they grab antibiotic molecules as they enter the cell and actively eject them back out before they reach effective intracellular concentrations. The most clinically dangerous efflux systems are non-specific: they can expel multiple different antibiotic classes simultaneously, which is why efflux pump overexpression often produces multidrug-resistant (MDR) organisms in a single step.
Why is MRSA resistant to beta-lactam antibiotics?
MRSA (Methicillin-resistant Staphylococcus aureus) carries a gene called mecA that encodes a modified penicillin-binding protein called PBP2a (also written as PBP2′). Normal penicillin-binding proteins are the enzymes that beta-lactam antibiotics bind to in order to block bacterial cell wall synthesis. PBP2a has an extremely low affinity for virtually all beta-lactam antibiotics — the drug simply cannot bind tightly enough to inhibit PBP2a. Because bacteria need PBPs to build their cell walls, and because PBP2a is unaffected by beta-lactams, MRSA can keep building its cell wall perfectly well even in the presence of these antibiotics.
How does horizontal gene transfer spread antibiotic resistance between bacteria?
Horizontal gene transfer (HGT) allows bacteria to share DNA during their own lifetime — not just to their offspring. There are three main routes: (1) Conjugation, where two bacteria make direct contact and one transfers a resistance-encoding plasmid to the other — this is the most important route clinically and can spread resistance extremely rapidly; (2) Transformation, where a bacterium takes up free DNA fragments from its environment, often from dead bacteria that have released their DNA; and (3) Transduction, where a bacteriophage (a virus that infects bacteria) accidentally packages resistance genes and transfers them to the next bacterium it infects.
Why are biofilms so resistant to antibiotics?
Biofilm resistance is multifactorial. First, the extracellular matrix of polysaccharides, proteins, and eDNA acts as a physical barrier that slows or blocks antibiotic penetration. Second, bacteria deep inside biofilms exist in a state of very low metabolic activity — and many antibiotics (particularly those targeting cell wall synthesis or DNA replication) only work effectively on actively growing bacteria. Third, within biofilms, bacteria communicate via quorum sensing and can upregulate efflux pumps and other resistance mechanisms. Fourth, biofilms contain specialized “persister cells” — a small subpopulation of phenotypically dormant bacteria that are phenotypically tolerant to virtually all antibiotics and survive to repopulate the biofilm after treatment is stopped.