Quick Summary
- Normal sperm morphology describes how many sperm cells in a sample have a correctly shaped head, midpiece, and tail.
- Under the WHO 6th Edition manual, a semen sample is considered within the normal range when at least 4% of sperm show a typical shape using strict scoring rules.
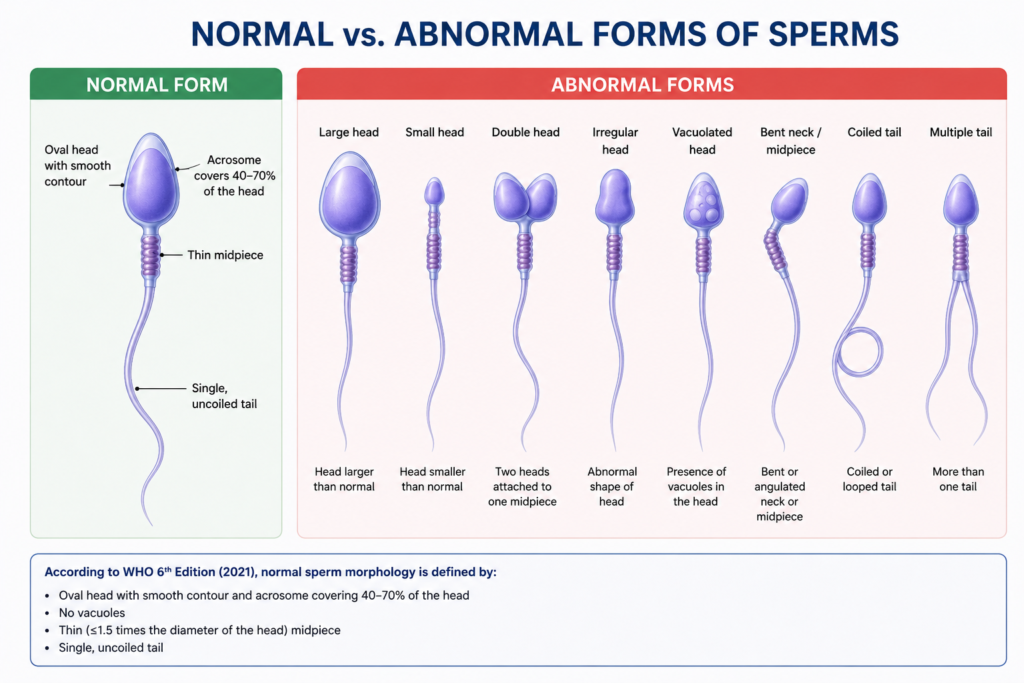
- A properly formed sperm cell has an oval head with a well-defined acrosome, a slender uniform midpiece, and a single straight tail.
- Falling below the 4% threshold is termed teratozoospermia, but a low percentage alone does not guarantee infertility.
- Morphology is scored under high magnification after staining, most commonly with a Papanicolaou-based technique.
- Shape defects can stem from genetics, infection, heat exposure, or lifestyle habits, and some are reversible.
- Morphology results are only meaningful when read together with sperm count and motility.
1. What Does "Normal Sperm Morphology" Actually Mean?
When a semen sample is examined under a microscope, not every sperm cell looks the same. Some have the expected smooth, oval head and straight tail; others are misshapen, oversized, undersized, or missing parts entirely. Normal sperm morphology is the term used to describe the proportion of cells in a sample that match the accepted shape standard for a healthy, functional sperm.
This is different from sperm count or motility. A man can have a high sperm count and strong swimming ability, yet still show poor morphology if a large share of those cells are structurally flawed. Because shape influences a sperm’s ability to swim efficiently and bind to an egg, morphology is treated as a quality marker rather than a quantity marker.
Grading criteria have tightened considerably since morphology was first studied. Early scoring systems were fairly forgiving and counted many borderline cells as acceptable. Today’s strict criteria — often called Kruger or Tygerberg criteria — are far less lenient, which is one reason the “normal” percentage looks so low compared to decades past.
2. Why Clinicians Look at Morphology in the First Place
A semen analysis is not run purely out of curiosity — the results guide real decisions about a couple’s fertility path. Morphology contributes to that picture in several ways:
- It offers a rough estimate of how likely sperm are to reach and fertilize an egg without medical assistance.
- It helps a clinician decide between natural timing, intrauterine insemination, or more intensive options like IVF or ICSI.
- Unusual patterns of misshapen sperm can point toward an underlying issue such as a varicocele, an infection, or a genetic condition.
- Repeat testing after treatment shows whether an intervention — medical or lifestyle-based — is actually improving sperm quality.
Multiple fertility studies have found that men whose normal-form percentage sits well below the reference cutoff tend to have measurably lower fertilization success during IVF cycles, which is why laboratories treat this number as more than a footnote.
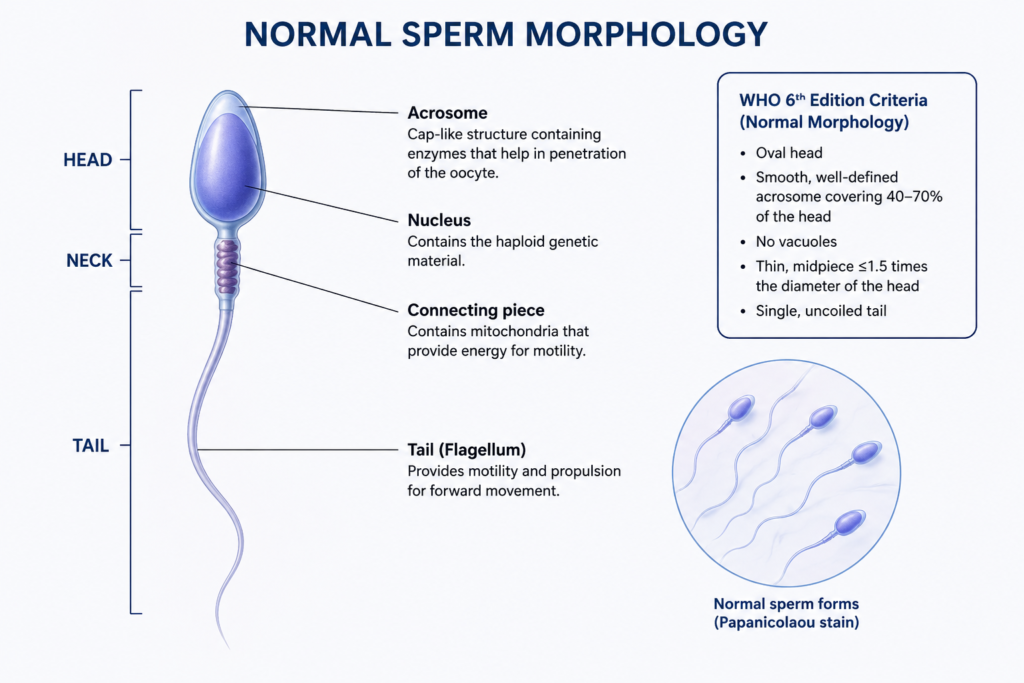
3. Anatomy of a Correctly Shaped Sperm Cell
To judge what counts as “abnormal,” an examiner first needs a clear picture of what “normal” looks like. A mature spermatozoon measures roughly 50–60 micrometers from end to end and is built from three connected sections.
3.1 Head
A normally shaped head is smooth and oval, generally around 4 micrometers long and just over half that in width. Inside sits the nucleus carrying the paternal DNA. Covering the front two-thirds of the head is the acrosome, a cap loaded with enzymes the sperm needs to break through the outer layer of the egg. The rear portion of the head, just behind the acrosome, contains factors involved in triggering the egg’s activation once fertilization begins.
3.2 Midpiece
Sitting just below the head, the midpiece is a short, slim connector roughly 4–6 micrometers long. It is wrapped in a spiral sheath of mitochondria — the cell’s energy generators — coiled around the central tail structure. Because this region supplies the fuel for movement, any thickening, bending, or asymmetry here tends to show up as sluggish or erratic swimming.
3.3 Tail
The tail, or flagellum, makes up most of the cell’s length at around 45 micrometers. Internally it relies on a bundle of microtubules arranged in a distinctive ring pattern, reinforced by supporting fibers. Coordinated flexing of this internal skeleton produces the whip-like beating motion that drives the sperm forward.
4. The WHO Reference Value for Normal Morphology
Laboratories worldwide rely on guidance published by the World Health Organization to standardize how semen samples are read. The current edition — the sixth edition, released in 2021 — replaced the 2010 fifth edition but kept the same strict approach to shape scoring.
Under this system, a sperm only counts as normal if the head, acrosome, midpiece, and tail all individually meet the defined shape standards at the same time. A cell that is borderline in even one region is scored as abnormal rather than given the benefit of the doubt.
Reference Threshold (WHO 6th Edition, 2021)
The lower limit for a normal result is 4% or more normally shaped forms, based on data from the 5th percentile of men with proven fertility. Anything below that figure is labeled teratozoospermia.
This same 4% cutoff was already in place under the 2010 manual. Older editions from the 1990s used far more relaxed criteria, with acceptable ranges as high as 14% or even 30%, so comparing historical results against modern ones requires caution.
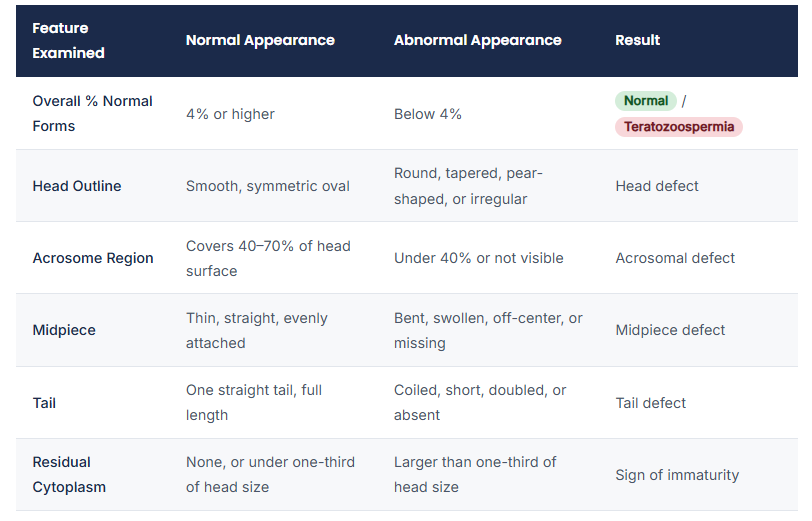
5. Normal vs. Abnormal Forms at a Glance
6. How a Normal Morphology Reading Is Obtained in the Lab
6.1 Preparing the Sample
Samples are typically collected after two to seven days without ejaculation, using a clean, non-toxic container. Before anything is examined, the semen is left to liquefy at body temperature for around 15–30 minutes. If liquefaction is incomplete, the smear can be distorted and the resulting count unreliable.
A thin film of semen is then spread on a clean glass slide and allowed to air-dry quickly. Slides that dry too slowly tend to show artificially stretched or shrunken cells, which throws off the morphology score.
6.2 Staining the Slide
Different stains bring out different levels of structural detail:
- Modified Papanicolaou stain: The technique WHO recommends as the reference method, giving sharp contrast between the nucleus, acrosome, and tail.
- Diff-Quik (a Giemsa-type stain): Faster and simpler, commonly used where high sample turnover is needed.
- Shorr’s stain: A multi-color alternative popular in some regional labs.
- Ready-made kits (e.g., SpermBlue): Pre-formulated stains designed for consistent, quick results.
6.3 Counting and Scoring
Scoring is done under oil-immersion magnification, usually at 1000x. WHO guidance calls for examining at least 200 sperm per slide to keep the margin of error near 5%; counting closer to 400 cells tightens that margin further. Each cell examined is marked normal or abnormal, and the specific defect type is logged for cells that fail.
7. Reading the Result: What Different Percentages Suggest
📊 General Interpretation Guide
- 4% or above: Within the expected range; morphology is unlikely to be the main fertility obstacle if other parameters are also fine.
- 1–3%: Reduced normal forms; natural conception odds drop, and clinicians often discuss IUI or IVF with ICSI.
- Under 1%: Marked reduction; ICSI is usually the recommended path, sometimes alongside genetic evaluation.
It’s worth stressing that morphology never stands alone. A man with a slightly low normal-form percentage but strong count and motility often has better real-world prospects than one with combined problems across all three parameters — a pattern sometimes referred to as OAT (oligoasthenoteratozoospermia).
8. What Can Lower the Percentage of Normal Forms
A below-threshold result is rarely traced to one single cause. Common contributors include:
- Varicocele: Enlarged veins around the testicle that raise local temperature and disrupt sperm formation — one of the few surgically fixable causes.
- Infection: Bacterial infections in the reproductive tract can generate oxidative stress that damages developing sperm.
- Heat exposure: Frequent hot tub use, tight clothing, or occupational heat can push scrotal temperature above the optimal range.
- Hormonal imbalance: Low testosterone, thyroid problems, or elevated prolactin can interfere with normal sperm development.
- Toxin exposure: Certain medications, chemotherapy, pesticides, and heavy metals are known to disrupt sperm shape.
- Diet and lifestyle: Smoking, heavy drinking, obesity, and poor nutrition are all linked with lower morphology scores.
- Unexplained cases: In a notable share of cases, no clear cause is ever identified.
9. Can Morphology Improve Over Time?
Because sperm are continuously produced, morphology is not a fixed, permanent trait. A full cycle of sperm development takes roughly two to three months, so changes made today typically won’t show up in test results for at least that long. Addressing an underlying issue — surgically correcting a varicocele, clearing an infection, or improving diet and reducing heat exposure — has been shown to nudge morphology scores upward in many patients, though results vary from person to person.
For couples facing a persistently low percentage, assisted reproduction techniques such as ICSI largely sidestep the shape barrier altogether by allowing an embryologist to select and inject a single sperm directly into the egg, regardless of the sample’s overall morphology percentage.
10. Practical Tips for Supporting Healthy Sperm Shape
- Keep body weight in a healthy range through regular moderate exercise.
- Avoid prolonged exposure to heat sources near the groin, including saunas and laptops resting directly on the lap.
- Cut back on smoking and limit alcohol intake.
- Favor a balanced diet with plenty of fruit, vegetables, and antioxidant-rich foods.
- Manage chronic stress through activities like exercise or relaxation techniques.
- Choose breathable, loose-fitting underwear.
- Limit exposure to industrial chemicals, pesticides, and heavy metals where possible.
11. Conclusion
Normal sperm morphology is one piece of a larger fertility puzzle — not a standalone verdict on a man’s ability to conceive. A percentage below the WHO reference range is a signal worth investigating, not an automatic diagnosis of infertility, especially when count and motility remain healthy. For anyone reviewing a semen analysis report, the most useful approach is to look at morphology alongside the other parameters and discuss the full picture with a qualified clinician rather than fixating on a single number in isolation.
Frequently Asked Questions
Q1. What percentage is considered normal sperm morphology?
Using WHO’s current strict criteria, 4% or more normally shaped sperm is considered within the reference range. Below that, the result is labeled teratozoospermia.
Q2. Does low morphology always mean infertility?
No. A low percentage lowers the odds of natural conception but does not rule it out, particularly when sperm count and motility are otherwise normal.
Q3. How is morphology tested in a lab?
A semen smear is stained — most often with a Papanicolaou-based method — and examined under high magnification, with at least 200 sperm assessed against strict shape criteria.